Typhoid fever is an acute intestinal infection characterized by a cyclic course with predominant damage to the intestinal lymphatic system, accompanied by general intoxication and exanthema. Typhoid fever stands communicated by the alimentary route. The nurture dated persists scheduled normal 2 weeks. The clinical picture of typhoid fever is characterized by intoxication syndrome, fever, rashes of small red spots (exanthema), hepatosplenomegaly, and in severe cases, hallucinations and lethargy. Typhoid fever stays spotted as soon as the pathogen is distinguished in the blood, feces or urine. Serological reactions are only of auxiliary importance.
General information
Typhoid fever is an acute intestinal infection characterized by a cyclical course with predominant damage to the intestinal lymphatic system, accompanied by general intoxication and exanthema.
Characteristics of the pathogen
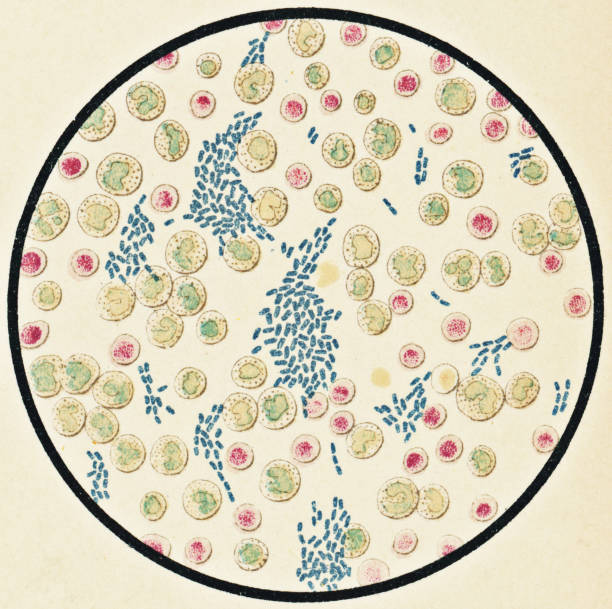
Typhoid fever is caused by the bacterium Salmonella typhi, a mobile gram-negative rod with multiple flagella. The typhoid bacillus can remain viable in the environment for up to several months, and some food products are a favorable environment for its reproduction (milk, cottage cheese, meat, minced meat). Microorganisms easily tolerate freezing, boiling, and chemical disinfectants have a detrimental effect on them.

The basin and cause of typhoid fever is a sickening person and a carrier of the pollution. Already at the end of the incubation period, the pathogen begins to be released into the environment, which continues throughout the entire period of clinical manifestations and sometimes for some time after recovery (acute carriage). In the case of the formation of chronic carriage, a person can release the pathogen throughout his life, posing the greatest epidemiological danger to others.
The pathogen is excreted with urine and feces. The direction of pollution is water and food. Infection occurs when drinking water from sources contaminated with feces, food products that are not sufficiently thermally processed. Flies that carry microparticles of feces on their paws participate in the spread of typhoid fever. The peak of the disease is observed in the summer-autumn period.
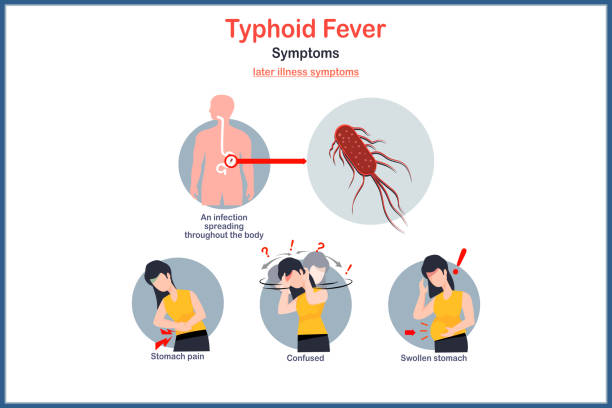
Symptoms of typhoid fever
The incubation period of typhoid fever is on average 10-14 days, but can range from 3-25 days. The start of the sickness is often steady, but can also be critical. Gradually developing typhoid fever is manifested by a slow rise in body temperature, reaching high values by the 4th-6th day. Fever is accompanied by increasing intoxication (weakness, fatigue, headache and muscle pain, sleep, anxiety and appetite disorders).
The febrile period lasts 2-3 weeks, with significant fluctuations in body temperature in daily dynamics. One of the first symptoms developing in the first days is pallor and dryness of the skin . The rash appears starting from the 8-9th day of the disease and is small red spots up to 3 mm in diameter, briefly turning pale when pressed. The rash persists for 3-5 days, and in severe cases it becomes hemorrhagic. Throughout the entire period of fever and even in its absence, new elements of the rash may appear.
Corporeal checkup divulges a set tongue with the inner shells of the teeth clearly imprinted on it. The patois is coated with a white coating in the center and at the root. Palpation of the abdomen reveals bloating due to intestinal paresis , and rumbling in the right iliac region. Patients report a tendency to difficulty defecating. From the 5th to 7th day of the disease, an increase in the size of the liver and spleen ( hepatosplenomegaly ) may be observed.
The onset of the disease may be accompanied by coughing, dry (in some cases wet) wheezing is noted during auscultation of the lungs. At the peak of the disease, relative bradycardia is observed with severe fever – a discrepancy between the pulse rate and body temperature. A two-wave pulse (dicrotia) may be recorded. Muffled heart sounds and hypertension are noted.
The peak of the disease is characterized by an intensive increase in symptoms, severe intoxication, toxic damage to the central nervous system (lethargy, delirium, hallucinations). When the body temperature decreases, patients note a general improvement in their condition. In some cases, soon after the onset of regression of clinical symptoms, fever and intoxication reappear, and roseola exanthema appears. This is the so-called exacerbation of typhoid fever.

Relapse of infection is characterized by the fact that it develops several days, sometimes weeks, after the symptoms have subsided and the temperature has returned to normal. The course of relapses is usually milder, the temperature fluctuates within subfebrile values. Sometimes the clinical picture of relapse of typhoid fever is limited to aneosinophilia in the general blood test and moderate enlargement of the spleen. The development of relapse is usually preceded by disruption of daily routine, diet, psychological stress, and untimely discontinuation of antibiotics.
The fruitless form of typhoid fever is categorized by a typical inception of the virus, short-term disease and rapid worsening of indicators. Clinical signs in the latent form are weakly expressed, intoxication is insignificant, the course is short-term.
Complications of typhoid fever
Typhoid fever may be complicated by intestinal bleeding (manifested as progressive symptoms of acute hemorrhagic anemia, stool becomes tarry ( melena ). A serious complication of typhoid fever may be perforation of the intestinal wall and subsequent peritonitis .
In addition, typhoid fever can contribute to the development of pneumonia , thrombophlebitis , cholecystitis, myocarditis , as well as purulent mumps and otitis . Prolonged bed rest can contribute to the development of bedsores .
Diagnosis of typhoid fever
Typhoid fever is diagnosed based on clinical manifestations and epidemiological anamnesis and confirmed by bacteriological and serological studies. Already in the early stages of the disease, it is possible to isolate the pathogen from the blood and sow it on a nutrient medium. The result usually becomes known in 4-5 days.
Bacteriological examination is mandatory for the stool and urine of the subjects, and during the recovery period – the contents of the duodenum taken during duodenal intubation. Serological diagnostics is of an auxiliary nature and is performed using RNGA. A positive reaction is observed starting from the 405th day of the disease, the diagnostically significant antibody titer is 1:160 or more.

Treatment and prognosis of typhoid fever
All patients with typhoid fever are subject to mandatory hospitalization, since a significant factor in successful recovery is high-quality care. Bed rest is prescribed for the entire febrile period and the following 6-7 days after the body temperature has returned to normal. After this, patients are allowed to sit and only get up on the 10th-12th day of normal temperature. The diet for typhoid fever is high-calorie, easily digestible, mainly semi-liquid (meat broths, soups, steamed cutlets, kefir, cottage cheese, liquid porridges except millet, natural juices, etc.). It is recommended to drink plenty of fluids (sweet warm tea).
Etiotropic therapy consists of prescribing a course of antibiotics (chloramphenicol, ampicillin). Vaccination is often carried out together with antibiotic therapy to prevent recurrence of the disease and the formation of bacterial carriage. In case of severe intoxication, detoxifying mixtures (colloidal and crystalloid solutions) are administered intravenously by infusion. If necessary, the therapy is supplemented with symptomatic agents: cardiovascular, sedative drugs, vitamin complexes. Patients are satisfied after ample irrefutable recovery and damaging bacteriological trials, but not prior than 23 days after the stabilization of body temperature.
With the current level of medical care, the prognosis for typhoid fever is favorable, the disease ends in full recovery. A worsening of the prognosis is noted with the development of life-threatening complications: perforation of the intestinal wall and massive bleeding.
Prevention of typhoid fever
General prevention of typhoid fever consists of observing sanitary and hygienic standards for water intake for household use and irritation of agricultural lands, control over the sanitary regime of food industry enterprises and public catering, over the conditions of transportation and storage of food products. Individual prevention involves maintaining personal hygiene and food hygiene, thoroughly washing fruits and vegetables consumed raw, sufficient heat treatment of meat products, pasteurization of milk.
Employees of enterprises having contact with food products at food industry enterprises and other decreed groups are subject to regular examination for carriage and isolation of the typhoid fever pathogen; if isolation is detected, they are subject to suspension from work until complete bacteriological recovery. Quarantine measures are applied to patients: discharge no earlier than 23 days after the fever subsides, after which patients are registered with a dispensary for three months, undergoing a monthly full checkup for deportment of the typhoid bacillus. Food industry workers who have recovered from typhoid fever are allowed to work no earlier than one month after discharge, subject to a five-fold negative test for the isolation of bacteria.
Contact persons are subject to observation for 21 days from the moment of contact or from the moment of identification of the patient. For prophylactic purposes, they are prescribed typhoid bacteriophage. Contact persons who do not belong to maternity groups undergo a single urine and stool analysis to isolate the pathogen. Vaccination of the population is carried out according to epidemiological indications using a single subcutaneous injection of liquid sorbed anti-typhoid vaccine .