Coronary Artery Aneurysm stands a expansion of the lumen of a coronary pitcher by 50% or more family member to its proximal segment. The leading causes of the pathology are atherosclerosis, systemic vasculitis, congenital anomalies, injuries and iatrogenic interventions. Coronary Artery Aneurysm is asymptomatic for a long time, heart pain and other clinical manifestations are observed in the case of coronary heart disease. To diagnose a vascular anomaly, angiography, ECG and ultrasound of the heart, a set of laboratory tests are performed. Cardiac surgical procedure (stenting, aneurysmectomy) is indicated for large aneurysms and difficulties.
General information
The pervasiveness of coronary blood vessel aneurysms (CAA) in the populace ranges from 0.4% to 5.4%. Coronary artery spread in statistical data is due to the absence of clinical symptoms of the disease and its late diagnosis. Coronary Artery Aneurysm pathology is common in all age groups, including children. Men are more often affected than women. The clinical significance of coronary aneurysms remains a controversial issue among scientists and doctors, since in some cases the vascular anomaly does not manifest itself in any way, while in others it causes acute cardiovascular events.
Reasons
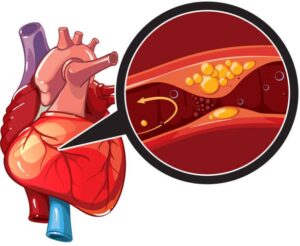
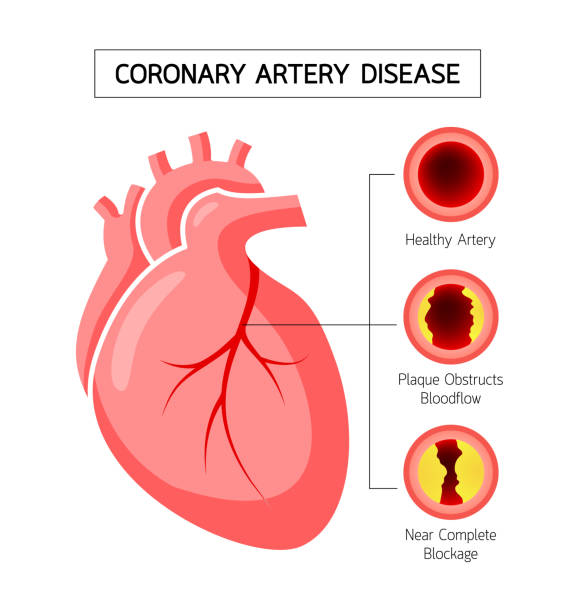
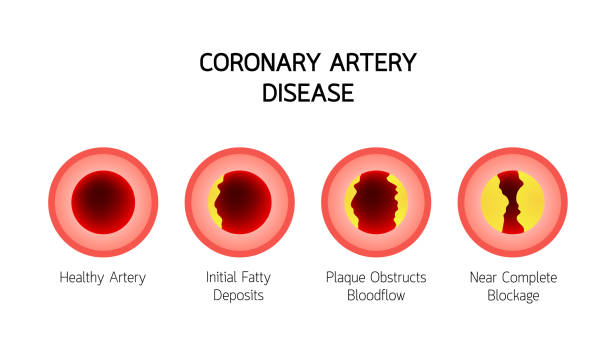
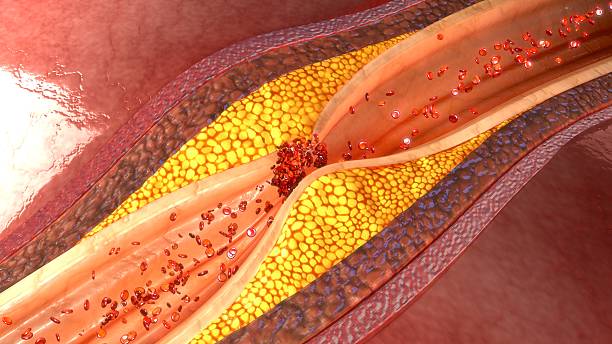
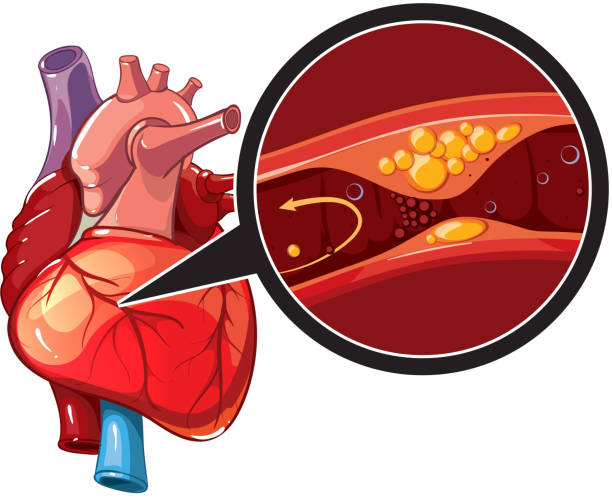
The main risk factor is recognized as atherosclerosis , which causes up to 50% of ACA. With the deposition of lipid plaques in the coronary vessels and progressive changes in the vascular wall, local expansion and bulging of the artery section is possible. Coronary Artery Aneurysm pathology often develops in people with a long history of atherosclerosis, the presence of concomitant hypertension , and a hereditary predisposition to cardiovascular diseases. Other causes of aneurysms:
- Systemic vasculitis . Up to 20% of cases of the Coronary arteryare associated with inflammatory changes in the vascular walls in Kawasaki disease, Wegener’s granulomatosis, Takayasu arteritis. Such pathologies can cause aneurysmal vasodilation in children and young people.
- Congenital anomalies. The pathology is associated with various disorders of the formation of the heart and vascular bed in the prenatal period. Predisposing factors for this condition have not been established; it is often combined with fibromuscular dysplasia.

- Mechanical damage. Pathological dilation of the coronary vessel is observed in some patients after chest injuries. Another cause is iatrogenic injuries – damage to vessels during aortocoronary bypass surgery, installation of stents without drug coating.
- Cocaine addiction . Cocaine has a direct damaging effect on the endothelium of the coronary arteries, disrupts blood flow and contributes to the development of vascular anomalies. An additional risk factor is repeated episodes of vasoconstriction and hypertension during drug intoxication.
In case of combined aneurysms of the coronary arteries, aorta and other main vessels, aneurysmal disease ,arrhythmia , artial fibrillation , is diagnosed. This pathology is typical for patients who have several groups of risk factors at once: genetic (presence of aneurysms in close relatives), cardiovascular (previous myocardial infarction , heart failure, stenosis of the carotid arteries ), atherosclerotic (high levels of LDL, apolipoprotein A1).
Pathogenesis
Pathological dilation of Coronary Artery Aneurysm in the arterial bed is associated with the combined action of several factors: chronic inflammation, atherosclerotic degenerative changes, increased blood flow velocity and increased blood filling of the coronary artery. Changes in the level of tissue metalloproteinases associated with a violation of the integrity of the vascular walls are of great importance in the pathogenesis of ACA.

Vascular anomaly provokes local circulatory disorders in the affected area, turbulent blood flows, and an increased risk of thrombus formation. Thromboembolic difficulties are conceivable after a thrombus or unsound plaque discontinuities off. Another negative aspect of ACA is the ineffectiveness of collateral circulation, which causes serious concerns in the case of concomitant atherosclerotic lesions of another coronary artery.
Classification
To establish Coronary Artery Aneurysm a diagnosis and choose a rational treatment strategy in practical cardiology, several options for systematizing coronary aneurysms are used. The disease is confidential according to the following landscapes:
- Form. Aneurysmal dilations of arteries are divided into 2 large groups: saccular, which can be single-chambered or multi-chambered, and spindle-shaped (fusiform).
- Number. Single aneurysms are more often observed in patients with atherosclerosis or previous intervention on coronary vessels. Multiple pathologies are characteristic of systemic inflammatory processes.
- systemic inflammatory processes.
- Size. According to the internal diameter, AKA are divided into small (up to 5 mm), medium (5-8 mm), giant (over 8 mm).
- Localization. More than 40% of anomalies are located in the right coronary artery, less frequently there is damage to the circumflex and descending branches of the left coronary artery. Expansion of the common trunk of the left coronary artery and three-vessel damage are casuistic cases.
Symptoms of Coronary Artery Aneurysm
In the case of a single vascular anomaly, there are no clinical manifestations. The diagnosis is most often made in middle-aged and elderly patients who are prescribed an angiographic examination of the coronary arteries in the presence of signs of angina . Multiple Coronary Artery Aneurysm are manifested by attacks of compressive chest pain that occur in connection with emotional shock or physical exertion.
Complications
The presence of a coronary artery aneurysm is recognized by many specialists as a factor in increasing the risk of myocardial infarction. Coronary Artery Aneurysm situation is complicated by concomitant atherosclerosis, arterial hypertension, and metabolic syndrome. In case of Coronary Artery Aneurysm giant vascular anomalies, extensive transmural infarction with cardiogenic shock is possible . In rare cases, spontaneous rupture of the affected vessel with the formation of hemopericardium and cardiac tamponade is observed .
Diagnostics
During a animal check by a cardiologist, not any precise ciphers of an aneurysm are perceived. If the patient has Coronary Artery Aneurysm or arterial hypertension, accents of heart sounds, functional and organic intracardiac murmurs, and other symptoms of cardiovascular pathology are determined. Also, anthropometric limitations are leisurely and BMI is calculated to weigh the risk of primitive obesity. The following methods are prescribed to diagnose ACA:
- Coronary angiography . X-ray examination of the coronary arteries with contrast is the “gold standard” for determining the presence, type and size of an aneurysm. Diagnostics are performed on all patients with suspected ACA and symptoms of angina. If showed, the procedure is complemented with highly revealing CT angiography .
- Ultrasound with Dopplerography . The study shows the contractility of the myocardium, the nature of blood circulation and the state of the main vessels. Ultrasound diagnostics does not allow visualization of a coronary aneurysm, but it is necessary for a comprehensive assessment of the state of the cardiovascular system.
- ECG . Electrocardiography results are important for diagnosing ischemic lesions of the heart muscle, identifying acute coronary syndrome as a typical complication of coronary artery aneurysm. According to the cardiogram data, it is possible to detect signs of left ventricular hypertrophy caused by arterial hypertension.
- Laboratory tests. To identify the underlying cause of the aneurysm, a lipidogram is performed with determination of total cholesterol and lipoprotein fractions. An rise in acute-phase dials directs universal vasculitis. In case of episodes of chest pain, tests for troponin and other myocardial markers are prescribed.

Differential diagnostics
When a typical angiographic picture is detected, the diagnosis leaves no doubt. Difficulties arise when differentiating between different causes of ACA, the need to exclude systemic vasculitis, other autoimmune and idiopathic forms of vascular damage. To clarify the prerequisites for the formation of a coronary aneurysm, a consultation with a rheumatologist, chest X-ray , and extended immunological studies may be required.
Treatment of coronary artery aneurysm
In case of a small size of ACA and absence of symptoms, dynamic observation is indicated. To control the size of the aneurysm and the condition of the coronary arteries, annual coronary angiography, ultrasound of the heart, ECG are performed. Since the disease is often combined with atherosclerosis, such patients are prescribed a low-cholesterol diet and hypolipidemic therapy. In case of development of ACA against the background of vasculitis, etiopathogenetic treatment according to protocols is indicated.
Indications for surgical intervention in case of coronary artery aneurysm are its gigantic size, critical disturbances of blood flow in the coronary vessels, unstable angina and high probability of myocardial infarction. In such cases, aneurysmectomy or aneurysm plastic surgery is performed in combination with various types of bypass operations . Endovascular treatment is also possible – installation of a drug-coated wall.
Prognosis and prevention
Most cases of ACA have a favorable course and are detected accidentally during a cardiological examination. A less optimistic prognosis is for patients with multiple giant aneurysms, refractory dyslipidemia , and progressive systemic vasculitis. Prevention of coronary aneurysms consists of timely diagnosis and treatment of diseases that cause vascular anomalies.